
A 53-year-old girl with no substantial previous professional medical history introduced to the unexpected emergency section with a 3-working day background of double eyesight on leftward gaze. She to begin with offered to urgent care with a chief criticism of chest heaviness and issue that her blood tension was too superior, but was sent to the emergency section for even further cardiac and neurological analysis immediately after her urgent care provider discovered abnormal eye motion. She endorsed mild, intermittent problems connected with diplopia when on the lookout to the left. Nonetheless, she denied any blurry vision when seeking ahead. She denied any trauma or falls.
Actual physical Test
Vitals: Temp 36.7°C Heart rate 86 beats/min Respirations 18 breaths/min BP 150/82 mmHg O2 Saturation: 100%
Typical: No acute distress and appears at ease. She is warn and oriented.
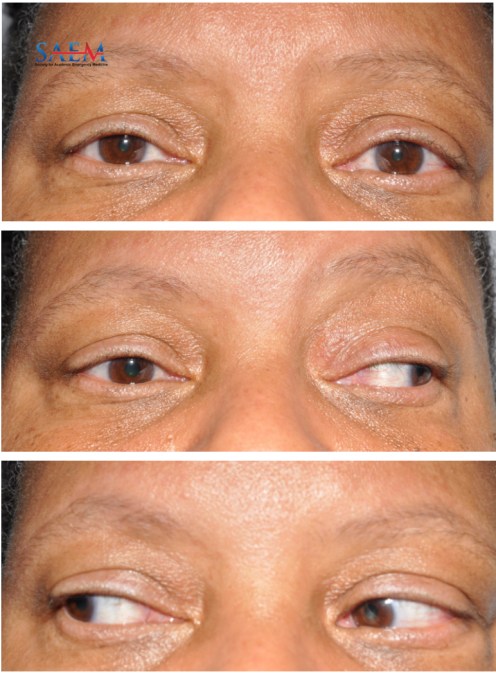
Eyes: Equivalent, round and reactive pupils and severely minimal adduction of the right eye, all other extraocular movements are standard.
Neuro: All other cranial nerves are intact, regular tone in bilateral upper and lessen extremities, regular sensation bilaterally to light touch and pinprick besides for mildly reduced feeling to pinprick around ideal ulnar distribution.
Laboratory Data
CBC, CMP, EKG, and Troponins had been ordinary.
Lipid panel: Cholesterol 241 (H)
CSF: No oligoclonal bands, Protein 197 (H), Albumin 57 (H), IgG 16.3 (H)
Scenario Question: What are some doable brings about of this patient’s right-sided internuclear ophthalmoplegia?
Internuclear ophthalmoplegia (INO) is outlined as the inability to adduct the eye due to a lesion in the medial longitudinal fasciculus (MLF) and can be accompanied by nystagmus in the similar eye. The two principal results in of internuclear ophthalmoplegia are demyelination of the medial longitudinal fasciculus (MLF) from many sclerosis (MS) and ischemic cranial nerve destruction from stroke. Even so, a in depth checklist of leads to of INO contains: infarction (ischemic stroke), demyelination (MS), tumor, encephalitis, hemorrhage, hydrocephalus, Chiari malformation, an infection (Lyme Condition), and trauma. Commonly, MS is found in more youthful patients where the two eyes are afflicted while strokes occur additional frequently in more mature clients and only just one eye is affected.
Case Problem: What labs and imaging can aid in the analysis of this client?
The therapeutic tactic focuses on treating the fundamental cause and that’s why pinpointing the etiology is of huge relevance. A mind MRI should really be purchased to appraise for ischemia and demyelination. Proton density imaging is effective in identifying MLF lesions in several sclerosis. A lumbar puncture can also support rule out bacterial infections. A kappa-totally free light-weight chain antibody examination is a speedier and much less pricey way to test for numerous sclerosis than searching for oligoclonal bands in the CSF.
Supplied this patient’s comparatively young age and vascular danger elements, stroke is optimum on the differential. Her mind MRI showed places of limited diffusion in the ideal dorsal medial pons correlating with her exam. It also confirmed periventricular and subcortical white make any difference improvements which is a non-specific locating in continual modest vessel ischemic alterations vs underlying demyelinating sickness. This was adopted up with an MRI of her backbone that demonstrated C5-6 stenosis with affiliated wire edema and an added improving C3-4 lesion concerning for demyelinating illness. Her lumbar puncture discovered 3 nucleated cells and a protein of 197 but was deemed a traumatic tap. There had been no oligoclonal bands. The first brain MRI conclusions favored stroke for which she underwent a stroke do the job-up and was eventually discharged on aspirin and atorvastatin for secondary avoidance. On the other hand, owing to concern for demyelinating illness, she was also handled with a 3-day course of IV methylprednisolone. Eventually, she was discharged and asked to come back again for a observe-up for repeat mind imaging and analysis. A the latest examine confirmed that clients with unilateral or bilateral INO who skilled symptomatic diplopia had been normally managed by uniocular occlusion. A different circumstance report showed that a young person who offered with acute INO responded swiftly to cure with IV alteplase when administered inside of 2 several hours of the onset of signs or symptoms and resolution inside of 15 minutes. A circumstance sequence revealed that 1 in 5 clients failed to recuperate from an INO. Consequently, it is critical that a definitive workup is carried out to decide the etiology of the INO.
Scenario Dialogue
Consider-Household Details
- Mind MRI which include DWI is a practical diagnostic instrument for INO.
- Unilateral INO is extra often similar to ischemic/vascular will cause while bilateral INO is affiliated with MS.
References
- Kim SS, Lee MH, Ji C. Unilateral Internuclear Ophthalmoplegia Next Minor Head Personal injury. Korean J Neurotrauma. 2022 Oct 2418(2):329-334. doi: 10.13004/kjnt.2022.18.e64. PMID: 36381451 PMCID: PMC9634317.
- Mahawish KM, Aravind A. Acute onset internuclear ophthalmoplegia responsive to therapy with intravenous alteplase. N Z Med J. 2020 Might 22133(1515):119-121. PMID: 32438384.
- Simmons J, Rhodes M. Conservative and Surgical Administration of Unilateral and Bilateral Internuclear Ophthalmoplegia (INO)-A Retrospective Assessment. Br Ir Orthopt J. 2022 Nov 718(1):152-158. doi: 10.22599/bioj.280. PMID: 36420121 PMCID: PMC9650975.
Copyright
Visuals and instances from the Society of Educational Crisis Drugs (SAEM) Medical Images Show at the 2023 SAEM Annual Assembly | Copyrighted by SAEM 2023 – all rights reserved. Look at other circumstances from this Scientific Picture Collection on ALiEM.
Creator information

Snehal Bindra, BS
Health care Scholar
Vanderbilt University Professional medical Centre
|
The write-up SAEM Medical Visuals Collection: Seeing Double appeared initially on ALiEM.


